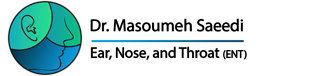
Thyroidectomy with Lymph Node Dissection
Thyroidectomy, which involves partial or complete removal of the thyroid gland, is one of the most common surgical procedures in modern medicine. This surgery is performed in conditions such as thyroid cancer, large goiters, suspicious thyroid nodules, or severe hyperthyroidism.
 When thyroidectomy is combined with removal of cervical lymph nodes, the complexity and clinical importance of the procedure increase significantly—especially in cases where thyroid cancer has metastasized to regional lymph nodes.
When thyroidectomy is combined with removal of cervical lymph nodes, the complexity and clinical importance of the procedure increase significantly—especially in cases where thyroid cancer has metastasized to regional lymph nodes.
This article provides a comprehensive overview of diagnostic steps, surgical techniques, potential challenges and complications, postoperative care, long-term follow-up, and related considerations to offer patients and families a clear understanding of this procedure.
Thyroidectomy and the Role of Lymph Nodes
The thyroid gland is a butterfly-shaped organ located at the front of the neck, just below the larynx. It produces the hormones thyroxine (T4) and triiodothyronine (T3), which regulate metabolism, body temperature, and heart rate. Adjacent to the thyroid are the parathyroid glands, which play a crucial role in regulating blood calcium levels.
Lymph nodes, distributed throughout the neck, are part of the lymphatic system and function to filter fluids, remove harmful substances, and support immune defense.
In conditions such as thyroid cancer—particularly papillary, follicular, or medullary types—cancer cells may spread through the lymphatic system to nearby lymph nodes.
This spread may present as palpable neck masses, abnormal swelling, or voice changes due to pressure on the recurrent laryngeal nerve. In some cases, lymph node involvement is asymptomatic and detected only through imaging studies. In such situations, thyroidectomy alone is insufficient, and lymph node removal becomes a necessary part of treatment to prevent disease progression.
Accurate Diagnostic Process
 Determining the need for thyroidectomy with lymph node dissection requires a multi-step diagnostic approach.
Determining the need for thyroidectomy with lymph node dissection requires a multi-step diagnostic approach.
The process begins with a physical examination of the neck to assess the presence, size, and characteristics of thyroid nodules and lymph nodes. Palpation may reveal abnormal enlargement or firmness.
Blood tests, including measurements of thyroid hormones (TSH, T3, T4) and calcitonin in suspected medullary thyroid cancer, provide initial information about thyroid function.
Imaging Studies
Imaging plays a vital role in diagnosis.
Neck ultrasound, a non-invasive and radiation-free method, is the first-line imaging modality for evaluating thyroid nodules and cervical lymph nodes.
CT scans and MRI provide more detailed information about tumor depth, vascular involvement, nerve proximity, and surrounding tissues.
When metastasis is suspected, PET scans or radioactive iodine scans may be used to detect distant disease spread.
Fine Needle Aspiration (FNA)
The next step is fine needle aspiration (FNA), in which a small tissue sample from the thyroid or lymph nodes is obtained using a thin needle and sent for pathological examination.
Biopsy results confirm whether a lesion is malignant and whether lymph nodes are involved, helping the surgeon determine the appropriate surgical approach—partial thyroidectomy, total thyroidectomy, or thyroidectomy with neck dissection.
Surgical Techniques and Approaches
Thyroidectomy with lymph node removal is a delicate procedure requiring advanced surgical expertise and careful planning. Depending on disease extent and patient factors, several techniques may be used:
Open Thyroidectomy
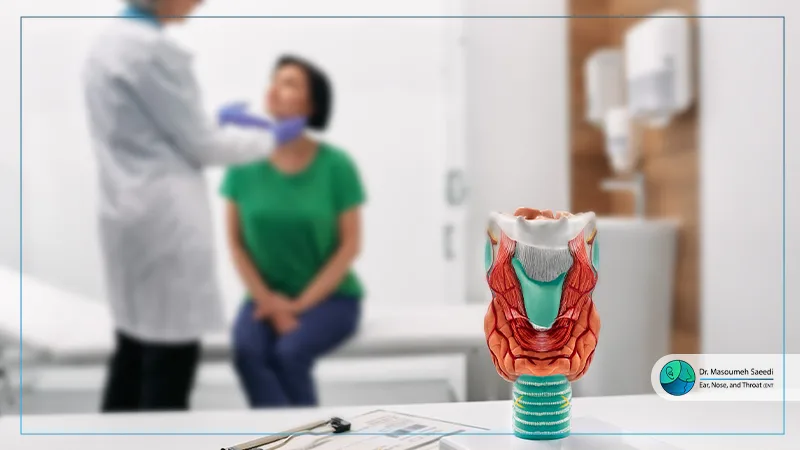
This traditional approach involves a horizontal incision at the lower neck, providing direct access to the thyroid gland and surrounding lymph nodes. The thyroid may be partially or completely removed, and suspicious lymph nodes excised if necessary.
This method is suitable for large tumors or advanced disease but may leave a noticeable scar.
Endoscopic or Robotic Thyroidectomy
These minimally invasive techniques use smaller incisions and advanced instruments such as endoscopes or robotic systems. They are ideal for patients with smaller tumors or those concerned about cosmetic outcomes. However, extensive lymph node removal may limit their use in advanced cases.
Neck Dissection
Neck dissection is specifically performed to remove lymph nodes and may be selective (removal of involved nodes only) or comprehensive (removal of all lymph nodes in a defined region, such as central or lateral neck compartments).
Because of proximity to vital structures—such as the carotid artery, jugular vein, and recurrent laryngeal nerve—this procedure requires exceptional precision.
To enhance safety, intraoperative nerve monitoring is often used to reduce the risk of nerve injury. Advanced imaging tools and microsurgical techniques also contribute to minimizing complications.
Challenges and Potential Complications
 Due to the complex anatomy of the neck, thyroidectomy with lymph node dissection carries certain risks.
Due to the complex anatomy of the neck, thyroidectomy with lymph node dissection carries certain risks.
One of the most common complications is injury to the recurrent laryngeal nerve, which may cause hoarseness, difficulty swallowing, or, in rare cases, permanent voice loss. This condition is often temporary but can become permanent in some patients.
Another potential complication is hypocalcemia (low blood calcium levels), resulting from damage to the parathyroid glands. Symptoms may include numbness, tingling in the hands and feet, muscle cramps, or seizures, requiring calcium and vitamin D supplementation.
Lymph node removal may also lead to lymphedema, where lymphatic fluid accumulates in the neck and causes swelling.
Other risks include intraoperative or postoperative bleeding, wound infection, and disease recurrence. In cancer cases, incomplete removal of malignant cells increases the risk of recurrence, making meticulous surgical technique and follow-up essential.
Patient age is also a factor: older individuals may experience longer recovery periods, while in children, ongoing physical growth can complicate surgical planning.
Postoperative Care and Recovery
The postoperative period is critical and requires close monitoring.
In the early days after surgery, pain management, infection prevention with prescribed antibiotics, and proper wound care are essential for optimal healing.
Patients who undergo total thyroidectomy must take lifelong levothyroxine therapy to replace lost thyroid hormones.
If laryngeal nerve injury occurs, speech therapy may be recommended to help restore voice function.
In cases of lymphedema, lymphatic massage or compression bandaging can reduce swelling.
Regular blood tests are performed to monitor calcium levels and thyroid hormone status.
Long-Term Follow-Up and Additional Treatments
Long-term follow-up is vital, especially in cancer patients. Periodic neck ultrasounds and, when indicated, imaging scans are used to detect disease recurrence.
A balanced diet, avoidance of heavy physical activity during the initial recovery weeks, and psychological support for patients and families contribute to faster and more effective recovery.
In selected cases, radioactive iodine therapy may be prescribed to eliminate remaining cancer cells and reduce the risk of recurrence.
Frequently Asked Questions (FAQ)
When imaging or biopsy confirms that thyroid cancer has spread to lymph nodes.
No. Lymph node removal depends on nodal involvement and is usually unnecessary in non-cancerous conditions.
Recovery typically takes several weeks to several months, depending on surgical extent and patient health.
Modern techniques minimize scarring, but complete disappearance is unlikely.
Through calcium and vitamin D supplementation under medical supervision and regular blood testing.
In most cases, no. Permanent voice changes occur only if nerve damage happens.
In non-cancerous conditions, medication or observation may be sufficient; surgery is essential in thyroid cancer.
The impact is usually minimal, though temporary swelling may occur.
It depends on cancer stage and completeness of tumor removal; regular follow-up reduces recurrence risk.
Yes, but it requires more careful planning and long-term follow-up due to growth considerations.
Most patients can resume normal activities within 2–4 weeks, depending on medical advice.
No. It is recommended only when there is a risk of remaining cancer cells.